
The Women’s Health Initiative (WHI): understanding hormone therapy & menopause
Why the Women’s Health Initiative was conducted
In 2002, the Women’s Health Initiative (WHI) dramatically changed how doctors and women thought about hormone replacement therapy (HRT), also known more recently as menopausal hormone therapy (MHT).
The WHI was one of the largest health studies ever conducted in women and aimed to understand how hormones influenced long‑term health risks such as heart disease, breast cancer, stroke and osteoporosis.
More than 160,000 postmenopausal women aged 50–79 participated in the study. One part of the trial examined hormone therapy. Researchers tested two types of treatment: combined oestrogen plus progestin therapy (for women with a uterus) and oestrogen‑only therapy (for women who had undergone hysterectomy).
In July 2002 the combined hormone therapy arm of the study was stopped early after researchers observed small increases in breast cancer, stroke and blood clot risk. The findings were widely reported in the media and many women stopped taking hormone therapy almost overnight.

The 2002 findings that changed menopause care
In July 2002 the combined hormone therapy arm of the study was stopped early after researchers observed small increases in breast cancer, stroke and blood clot risk. The findings were widely reported in the media and many women stopped taking hormone therapy almost overnight.
What researchers learned after re‑examining the WHI data
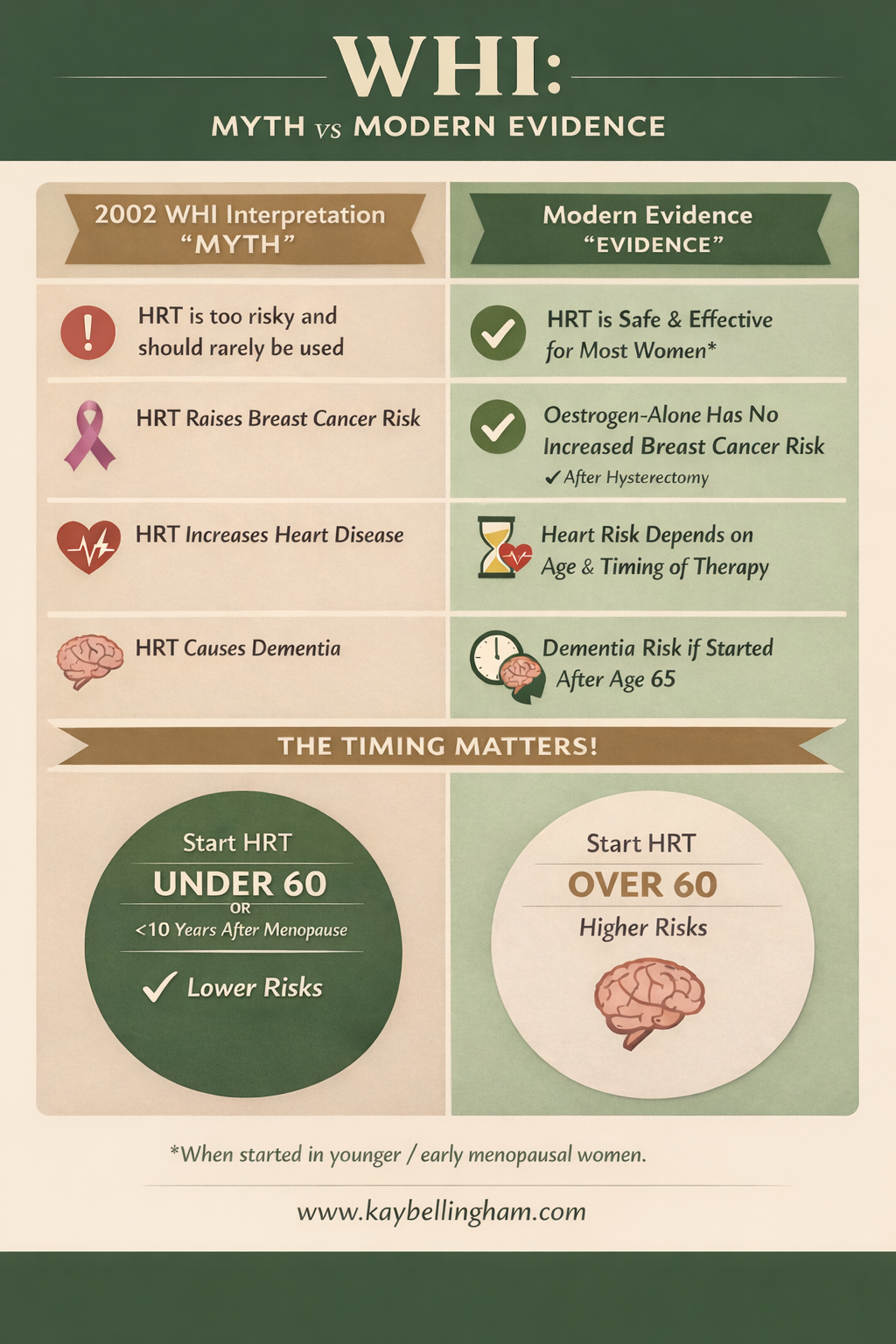
However, over the past two decades reseachers have revisited the WHI data and discovered that the interpretation was more complex than originally presented. A key insight was that age and timing of therapy are extremely important.
Most women in the WHI study started hormone therapy at an average age of 63, more than ten years after menopause. Today we know that starting hormone therapy closer to menopause often produces a different risk profile compared with starting later in life.
The ‘timing hypothesis’
Modern menopause research describes this as the ‘timing hypothesis’. Women who begin hormone therapy before age 60 or within 10 years of menopause generally experience a more favourable balance of benefits and risks.
Potential risks of hormone therapy
Like any medical therapy, hormone treatment has potential disadvantages. Combined oestrogen and progestin (synthetic form of progesterone) therapy may slightly increase breast cancer risk when used for long periods.
Hormone therapy can also increase the risk of blood clots or stroke in some women, particularly those starting treatment later in life.
Individualised menopause care
For this reason, menopause care today focuses on personalised decision‑making. A woman’s age, time since menopause, medical history and symptoms are all considered before starting therapy.
The WHI remains an important study because it helped clarify both the benefits and the risks of hormone therapy. Today the evidence supports a more balanced approach that helps women make informed decisions about managing menopause symptoms and long‑term health.
WHI timeline
1991 – The Women’s Health Initiative study begins in the United States
2002 – Combined oestrogen + progestin trial halted early due to risk signals
2004 – Oestrogen‑only trial stopped
2010–2020 – Re‑analysis of data introduces the 'timing hypothesis'
Today – Hormone therapy recognised as an effective treatment for menopausal symptoms when used appropriately
Understanding absolute risk vs relative risk
Relative risk and absolute risk are often confused in media reporting. Relative risk describes how much a risk increases or decreases compared with another group.
Example:
If breast cancer risk increases by 25%, this sounds alarming. This is the relative risk. Absolute risk looks at the actual number of people affected.
Example using WHI data:
Out of 10,000 women taking combined hormone therapy for one year:
• About 30 women developed breast cancer in the placebo group
• About 38 women developed breast cancer in the hormone therapy group
This means there were about 8 additional cases per 10,000 women per year.
While the relative increase appears large, the absolute increase is small. Understanding this difference helps women make more balanced decisions about treatment. Of course, no one wants to be a statistic, so it’s always advisable to look at all the options available to you.
References:
Rossouw JE et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women. JAMA. 2002.
Manson JE et al. Menopausal hormone therapy and long‑term outcomes of the Women’s Health Initiative trials. JAMA. 2013.
North American Menopause Society. 2022 Hormone Therapy Position Statement.
Pinkerton JV. Menopause and hormone therapy. Endocrine Reviews.